
Epidemic contagion is a cornerstone of how we think about the period of Native American encounters with European and African newcomers, roughly 1500-1850. As we live through a global pandemic, we are once again faced with life-changing, or life-taking, circumstances. The request for the new word neehseehpineenki ‘COVID-19’ begs the question: How important was disease in Myaamia history?
See also weehki-kaloosioni: neehseehpineenki ‘New Word: Breathing Illness (COVID)’
Myaamiaki and their neighbors experienced many recorded, and surely some unrecorded, instances of epidemics. Smallpox (or another pestilence) traveled to them in 1519-24 and 1639, each before any Myaamia person had met a European. Measles hit in 1633-34, decades before the first supposed meeting between European explorers and Miamis. The vectors are unknown–were Myaamia traders traveling to distant Atlantic ports? Probably. Did Native merchants pass ideas, trade items, and germs “down the line” to Myaamia towns? Almost definitely. European traders, soldiers, and missionaries also carried contagion.
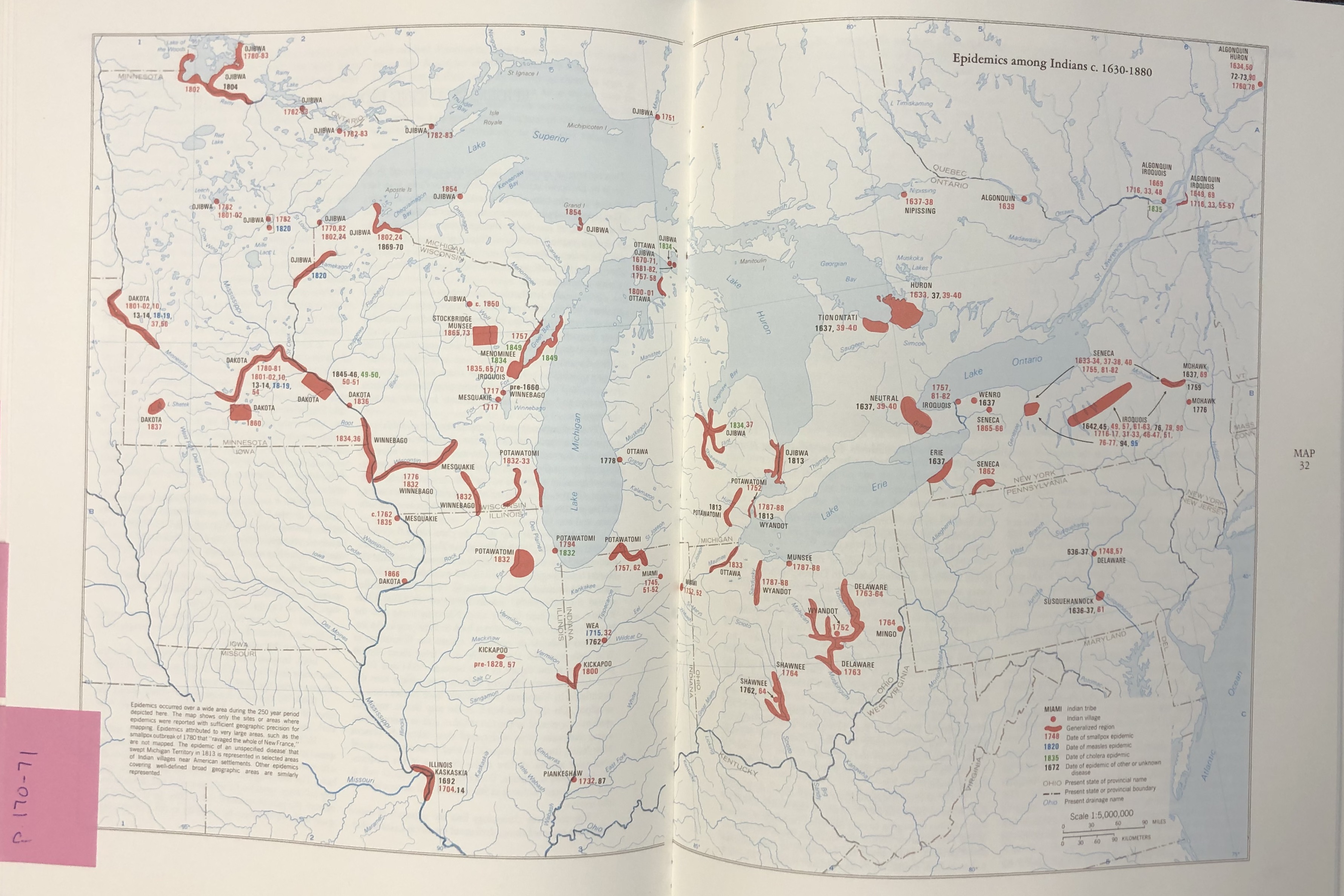
Survivors could be blinded or heavily scarred, such as Henri, a Kaskaskia man, around 1703. The local missionary noted: “He was attacked by smallpox, with all his family: this disease snatched from him at once his wife and some of his children; it rendered the others blind or extremely disfigured.”[1]At about this time, an unnamed (perhaps the same) plague attacked the Kickapoo, Mascouten, and Wea towns at Waayaahtanonki. It “desolated their Village, killing “many” every day.”[2] Measles hit Waayaahtanonki in 1715; a severe bout of smallpox struck the Miami-speaking villages in 1732-33. Families fled their towns to avoid it. Kiteepihkwanonki ’ was nearly obliterated; seven men survived.[3] At the beginning of the Seven Years’ War, smallpox appeared at Kiihkayonki and its satellite villages on the upper Tippecanoe and Eel Rivers, before spreading to Detroit and Wyandot villages near Lake Erie. And at the end of the Seven Years’ War, as smallpox spread among Miami-Illinois speakers and their neighbors, a Wea akima told a British traveler: “We assure you we are Rendered very miserable at Present on Account of a Severe Sickness that has seiz’d almost all our People, many of which have died lately, and many more likely to Die.”[4]
In 1796, the famed doctor Benjamin Rush administered smallpox inoculation to Mihšihkinaahkwa in Philadelphia.[5] Inoculation—actually variolation, which was rendered obsolete by vaccination—insured that the patient would not contract the pox in the future, but required inserting a smallpox scab or (in European practice) fluid from an infected individual underneath the skin of the patient, who would acquire smallpox in a controlled environment, sometimes under quarantine, and, with proper care of inoculated caregivers, survive it.[6][6] This practice was new in the British world, having been developed in Asia and passed to British medical practitioners both by West African slaves in New England and more recently to Great Britain’s medical literature via Turkish sources.[7] Mihšihkinaahkwa or one of his party carried the live pox culture back to Kiihkayonki to administer it to others to allow them to acquire immunity.[8]

At least five Miami children died during the removal to Kansas in 1846, and the community suffered from continual illness, despite an attendant physician.[9]
These too-brief sources help demonstrate some truths about past epidemics in Myaamionki— viruses impacted some communities more than others; we see waves of illness over generations; and Myaamia people sought to curb a plague’s effects with the knowledge that they had at the time.
In many ways, then, the current COVID-19 pandemic echoes past contagions, but I want to focus on the first truth—viruses and other contagious diseases hit some communities harder than others. This truth is significant in Myaamia history, because many of us have the general idea that European diseases swept the American continents, ravaging populations who had no exposure to smallpox, measles, influenza, and other communicable pathogens.
It is difficult to say with any degree of certainty how epidemics such as measles and smallpox impacted Myaamia demographics. For example, we do not know how many Myaamia people were alive in 1550 or 1650, and so it makes any post-contact trajectory difficult to determine. Yet, in the period 1750-1850, the Myaamia population dropped from perhaps 3,000 (including Weas and Piankeshaws) to about 500–a century that also included a forced removal, bloody wars, and in the nineteenth century, dependency on U.S. aid. Like some Native nations, perhaps the early years of European encounter actually coincided with population growth; we don’t currently know. But in the grand narratives of American history, many would attribute declining Native populations to germs. Most of my students at Miami University come to class “knowing” that epidemics basically wiped out a continent. They included a range of pathogens and symptoms in English variously called poxes, plagues, fevers, or fluxes,[10] or in Myaamia neehpikilokiinki ‘red skin’ (measles), neehpikaahkitiinki ‘bloody rear’ (dysentery), or meemahkilookiinki ‘bumpy skin’ (smallpox). In this version of American history, disease cleared a continent for European settlement.
This easy-to-digest narrative began with early modern colonization–albeit in that version, colonizers believed that God was clearing the landscape. This belief even found its way into the English charter for New England: “There hath, by God’s Visitation, reigned a wonderfull Plague… amongst the savages there Heertofore inhabiting, in a manner to the utter Destruction, Devastation, and depopulacion of that whole Territorye, so as there is not left … any that doe claime or challenge any Kind of Interest therein.”[11]
Since the 1970s, the explanation for why Native bodies seemed to succumb to diseases that their settler counterparts survived or avoided altogether has sought to apply scientific rather than spiritual causes. Alfred Crosby coined the term “virgin soil epidemics” to describe invasive microbes that came from Eurasia along with people, plants, animals, ideas, and technologies. Because Myaamia bodies (like all indigenous Americans) did not have previous experience with European, African, or Asian diseases, Myaamia people were “therefore immunologically almost defenseless.”[12] In this telling, Myaamionki was a “virgin soil” because Myaamiaki did not have experience with Eurasian pathogens; at least not at first contact. They had not acquired immunity. Crosby’s work in the environmental history of European expansion was revolutionary. But his ideas reached a popular audience in a streamlined and problematic way, in the form of Jared Diamond’s book, Guns, Germs, and Steel, which sought to explain why Europeans had conquered the globe (you can guess Diamond’s answer!). The question itself is deterministic, but the theory has become fact in the minds of many, and has found new life in the work of Charles Mann’s books, 1491 and 1493. Diamond stripped Crosby’s argument of its nuance when he wrote that “The main killers were Old World germs to which Indians had never been exposed, and against which they therefore had neither immune nor genetic resistance…Their destruction was accomplished largely by germs alone.”[13] In practice, this has translated to my students often coming to history class “knowing” that Native people had “no immunity” to diseases, and frequently assuming that no contagious diseases even existed in the Americas. Both are wrong; American Indians were and are born with similar antibodies to their human counterparts elsewhere, and tuberculosis, typhoid, streptococcus, and chickenpox, in addition to parasitic diseases, all preceded Europeans. The flawed notion that Europeans had “genetic resistance” to diseases too often translates to a kind of race-based superiority. In essence, the notion of “virgin soil epidemics” suggests that Europeans were naturally selected to survive, and Indians selected by nature to die. Of course, that ignores any human role in history.
In reality, health and society interact. Consider COVID-19: people living in poorer zip codes are acquiring and dying at higher rates than wealthier communities. Indigenous communities like Navajo Nation, or black and brown neighborhoods in Los Angeles and New York, are experiencing this pandemic more acutely than their neighbors.
What we are witnessing now supports revisions to “virgin soil” theory and, in turn, re-frames how we might understand disease in Myaamia history. Research in the last two decades, informed both by historians and medical professionals, has refined both the historical and biological forces at play. Here is the newer story: like smallpox or measles (two pernicious viruses in the colonial era), bodies who have survived COVID-19 (may be) prepared to combat future instances—that is, immune systems can fight the pathogen. That was the case for a person in 1720 Paris or London or Cairo or Kiihkayonki, no matter their “race.” Eighty to ninety percent of Europeans had survived smallpox, meaning that each body developed immunity, usually as a young child. On the other hand, on first contact and for generations thereafter, smallpox was not endemic in the Myaamia community. That meant that, if Myaamiaki and their neighbors experienced smallpox every thirty years, anyone under thirty years old had not survived smallpox and thus did not have immunity. The same was true for settlers born in the colonies—smallpox was not endemic in America, and so Miami people had similar immunity to smallpox as British colonists at the time of the American Revolution.

Biological “race” or genetics did not propel epidemics into Myaamionki. Social conditions did. Neither smallpox[14] nor COVID-19—despite some early assertions—were (are) equalizers. Instead, despite the basic similarities among human bodies, the disease is striking poor and disenfranchised communities at higher rates. For example, no serious person argues that different rates of infection for COVID-19 can be explained by the different genetics of, say a Wuhan resident versus a resident of Bergamo, or New York City. The Navajo Nation is experiencing higher rates of COVID-19 not because they are racially different than their neighbors, but almost assuredly because of the social determinants of health, such as under-resourced infrastructure.[15]
Recent news about incubation periods, social and physical distancing, and quarantines all echo similar ideas in Myaamia history. Myaamia people, like all people before modern medicine and science, did not know about . If someone acquired smallpox, they could pass the contagion as they traveled from home to home, or town to town, for a couple weeks before symptoms presented. Furthermore, like most people globally before the modern era, Myaamia families lived in close quarters and as extended families. Eating, sleeping, and chatting in confined spaces is no way to prevent an outbreak. (Imagine the intimacy of a sweat lodge, or even a wiikiaami on a winter’s night.)
So why did Myaamia people die at high rates from “virgin soil” diseases? Maybe the entire question is wrong-headed. Eighty percent of Jamestown colonists—saturated with European disease—died between 1607 and 1625, from a combination of poverty and malnutrition, contagion and other illnesses, and violence. Smallpox ravaged the Patriot army during the American Revolution.[16] Differential immunity does not explain these high figures; social and historical conditions do. In other words, diseases affect populations in context, today and yesterday.
Still, we know that epidemics swept across Myaamia towns many times in the past. But the above discussion hopefully clarifies that Myaamia vulnerability was caused by social stressors, poverty, malnutrition, lack of access to medicine or healthcare, migrations, violence, in-access to clean water, and variations in community or personal exposure.

Put another way, immunity was one part of a larger picture. Myaamia towns were not a world apart from our current predicament. Many were exposed to measles or smallpox or influenza, but the mortality rate was not 90% from infection alone, or close to 90% in any one plague. Rather, the initial shock of smallpox might have sapped resources. As adults became ill and unable to move, children and grandparents had to tend to the miincipahka ‘corn fields,’ to hunt moohsooki ‘White-tailed deer,’ and to carry nipi ‘water.’ (Dehydration is a particularly significant issue in many illnesses.) As healers tended to the sick, they themselves were vulnerable to infection and either stopped their medicine, or accidentally spread the pestilence from family to family. (High mortality among healthcare workers, such as miteewaki ‘shamans’ might have influenced the transmission of their specific knowledge, as well.) Pneumonia, or other diseases that can thrive in compromised bodies, sometimes claimed more lives. As the proportion of the sick in a community became larger, available labor for the health of the community lessened, potentially leading to malnutrition, dehydration, lack of childcare, and a decline in palliative care. And as the community experienced and recovered from the crisis, lower fertility rates may have influenced Myaamia population trends, as well.
Colin Calloway has summed up one effect of epidemiological disaster in our shared history. Taking the case of just one significant epidemic–smallpox spread across the continent 1779-1783–he writes: “The Revolution meant a new nation had its eyes on the West; smallpox cleared the West for occupation. George Washington crossing the Delaware is a more comfortable image of nation building than smallpox stalking Indian lodges, but they are two sides of the same coin in explaining how the West became ‘American.’”[17] Contagious disease is certainly a significant plotline in Myaamia history, but germs must be situated in community contexts.
What are the “lessons” we can apply today? I’m not sure. But for me, living through this present is helping me understand the past a bit better.
[1] Relation of Gabriel Marest, 1712, in Thwaites, ed., Jesuit Relations, 66: 247.
[2] Ibid. 239.
[3] Boishébert to Beauharnois, July 24 1733, in MPHS 34: 109; but see Joseph L. Peyser, “It Was Not Smallpox: the Miami Deaths of 1732 Reexamined,” Indiana Magazine of History 81, no. 2 (1985): 159-169. Because variolation resulted in actual infection, mortality was about 1-3%.
[4] Thomas Hutchins, journal in 1762, quoted in Charles Hanna, The Wilderness Trail, 2: 366. A geographic and chronological list of epidemics in the Great Lakes is in Tanner, Atlas of Great Lakes Indian History, 169-74.
[5] Paul A. Hutton, “William Wells: Frontier Scout and Indian Agent” Indiana Magazine of History 74, no. 3 (1978): 203. Mihšikinaakwa was recovering from smallpox when he, William Wells, and French philosopher Comte de Volney conversed in Philadelphia. Constantin François de Chassebœuf, comte de Volney, View of the Climate and Soil of the United States of America… (1804): 401.
[6] Elizabeth A. Fenn, Pox Americana: The Great Smallpox Epidemic of 1775-82 (New York: Hill and Wang, 2001). Variolation uses smallpox, variola, while vaccination uses the related cowpox, vaccinia.
[7] “The Fight over Inoculation during the 1721 Boston Smallpox Epidemic,” Science in the News Blog, Harvard University. <http://sitn.hms.harvard.edu/flash/special-edition-on-infectious-disease/2014/the-fight-over-inoculation-during-the-1721-boston-smallpox-epidemic/>; Fenner, et al, Smallpox and its Eradication (Geneva: World Health Organization, 1988), 256-58; Gulten Dinc and Yesim Isil Ulman, “The Introduction of Variolation ‘A La Turca’ to the West by Lady Mary Montagu and Turkey’s Contribution to This,” Vaccine 25 (2007): 4261-4265.
[8] Colin G. Calloway, The Indian World of George Washington: The First President, the First Americans, and the Birth of the Nation (New York: Oxford University Press, 2018), 461.
[9] Myaamiaki aancihsaaciki: A Cultural Exploration of the Myaamia Removal Route (Miami Tribe of Oklahoma, 2011).
[10] Pox from English, “to have pock-marks or pocks,” and flux derived from Latin “to flow.”
[11] The Charter of New England, 1620. <https://avalon.law.yale.edu/17th_century/mass01.asp>
[12] Alfred Crosby, “Virgin Soil Epidemics as a Factor in the Aboriginal Depopulation in America,” The William and Mary Quarterly 33, no. 2 (1976): 289.
[13] Diamond, 211-212; 322. The counterpoint to “virgin soils,” and the primary inspiration for this post, is David S. Jones, “Virgin Soils Revisited,” The William and Mary Quarterly 60, no. 4 (2003): 703-742.
[14] I am focusing on smallpox both because it was a repeat epidemic among the Myaamia, but also because it is so well known as a “virgin soil” virus. Other epidemics included measles, influenza, typhus, malaria, dysentery, and whooping cough, only some of which affected Myaamia bodies differently than non-Myaamia bodies.
[15] For examples, see the United Nations: “COVID-19 and Indigenous peoples” and the Centers for Disease Control and Prevention: COVID-19 in Racial and Ethnic Minority Groups.”
[16] Jones, “Virgin Soils Revisited,” 739-740.
[17] Colin G. Calloway, One Vast Winter Count: The Native American West Before Lewis and Clark (Lincoln: University of Nebraska Press, 2003), 426.
Related posts:

Leave a comment